
I am (DDS with MS in Specialized Orthodontics, and I am not an OFMS), often asked about TMJ anatomy, TMJ disorders (TMD), Idiopathic condylar resorption (ICR), Progressive condylar resorption (PCR) and Total TMJ replacement (TJR).
I have collected some information that may benefit both Medical Providers and patients.
Here is some basic information about TMJ, TMD, TMD diagnosis, ICR, and their treatment. This was not intended to be an exhausting list of information about TMD, but to be just a simple basic information guide based on published literature.
I will continue to update this post in the future, so please check back…
For more Q&A and info – feel free to join our Support group “Orthognathic Jaw surgery, condylar resorption, sleep apnea – Support group” – https://www.facebook.com/groups/121154992481515/
Some references:
Please learn the terminologies correctly.
Everyone has TMJ Temporomandibular joints, but not everyone has TMD Temporomandibular Joint Disorders.
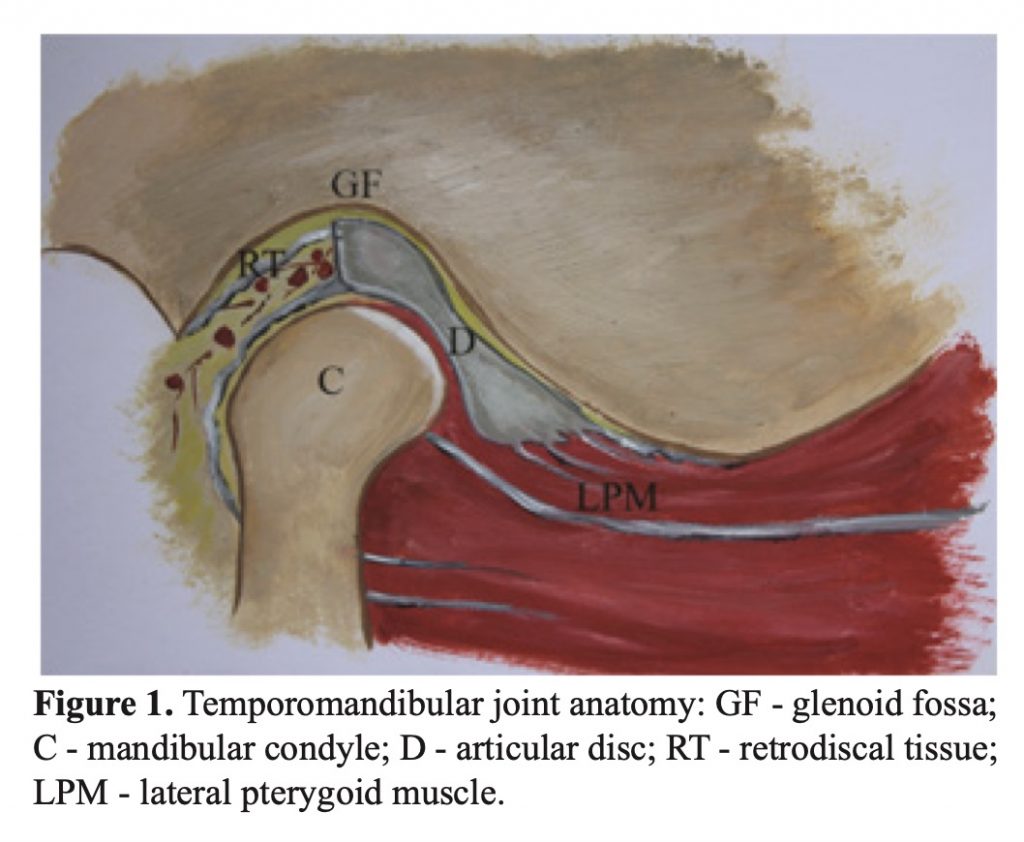
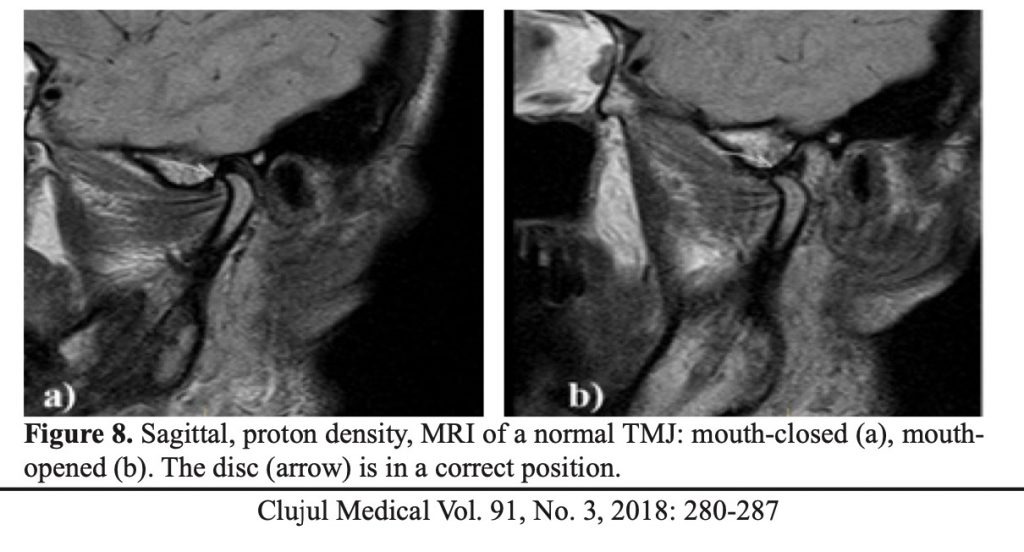
Here is a healthy TMJ
https://nagyorthodonticacademy.com/wp-content/uploads/2020/01/cm-91-280.pdf
Normal TMJ – Temporomandibular joints
TMD Temporomandibular Joint Disorders – Diagnosis and Imaging.
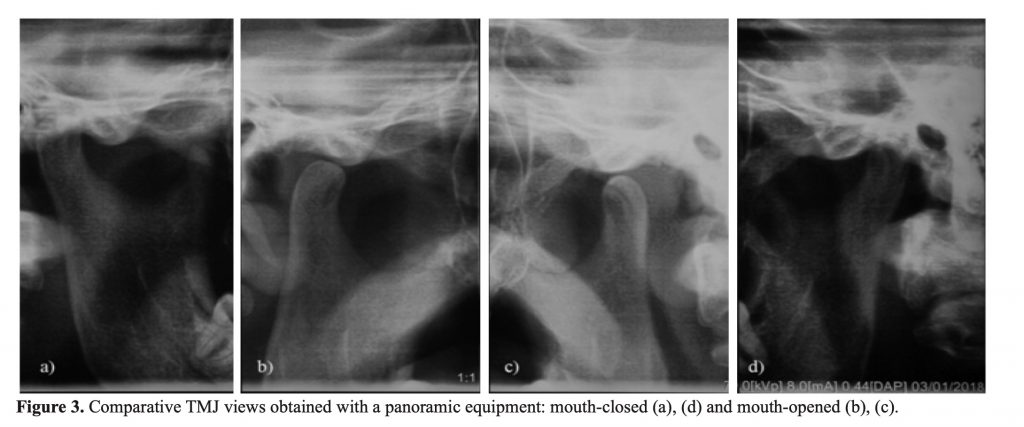
- X-rays.

TMJ image from PAN
Ceph

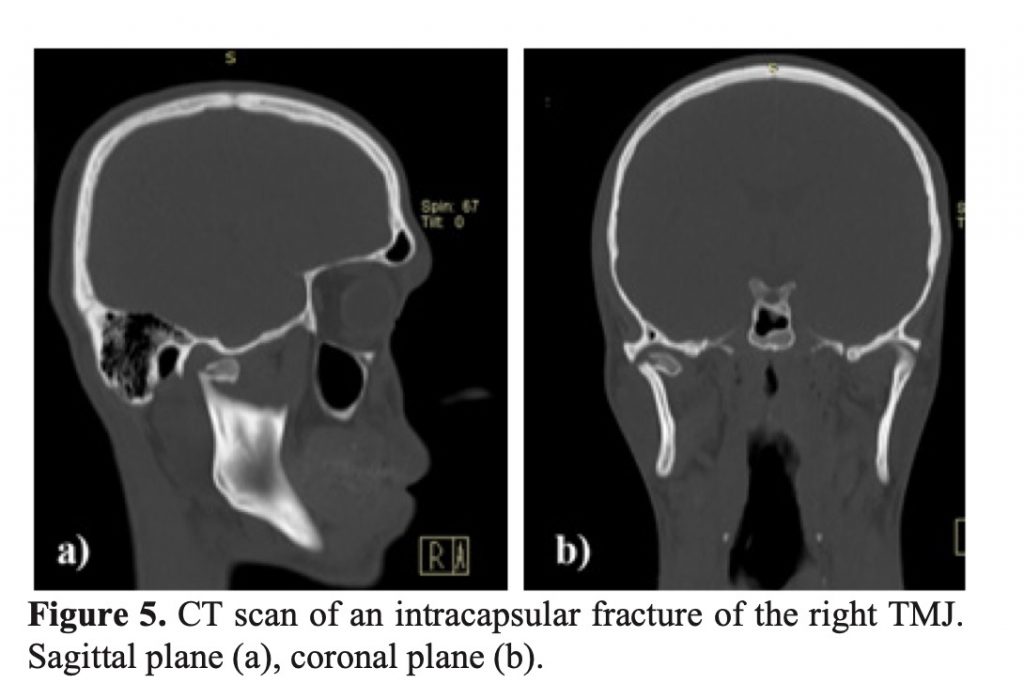
2. CT

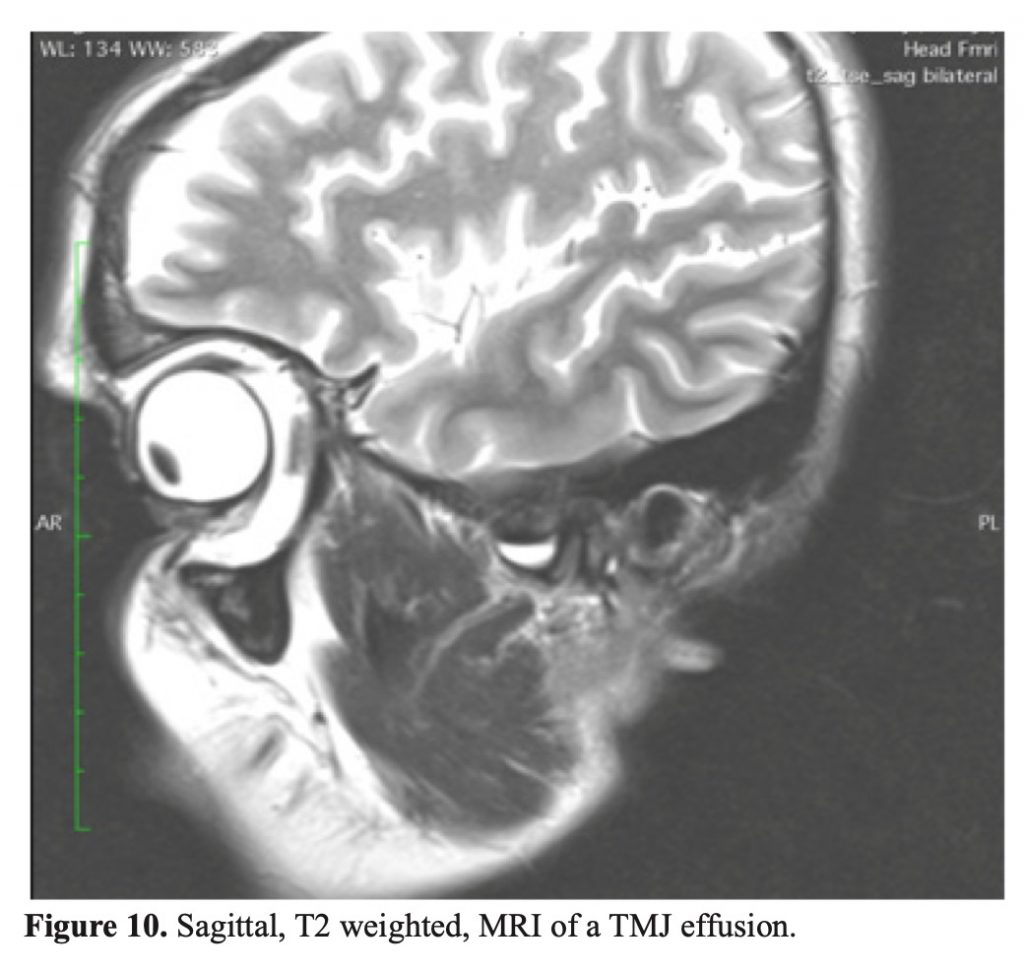
3. MRI

4. Ultrasound (US). I think ultrasound will be an even more utilized diagnostic tool for TMD diagnosis as ultrasounds get more sensitive and clear. USs can be used during movements, they are inexpensive, portable, and are very noninvasive, so their use would be desirable. Image quality is still an issue, and during opening sometimes it’s hard to see the subject clearly.
Temporomandibular Joint Disorders – TMD
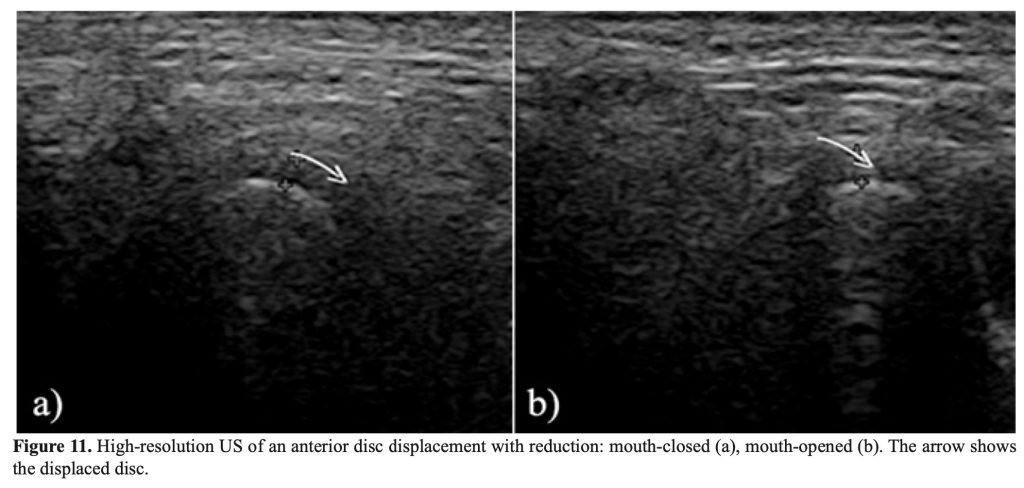
This is what happens when a patient opens, and they hear a click. This can happen after trauma, normal growth, or due to class II forward posturing and other issues.
Treatment: Sometimes full mouth occlusal adjustments, short term (1-3-6 months) of splint therapy – ONLY as a temporary solution, anti-inflammatories. Some cases resolve after some time, others stay the same or even get worse.
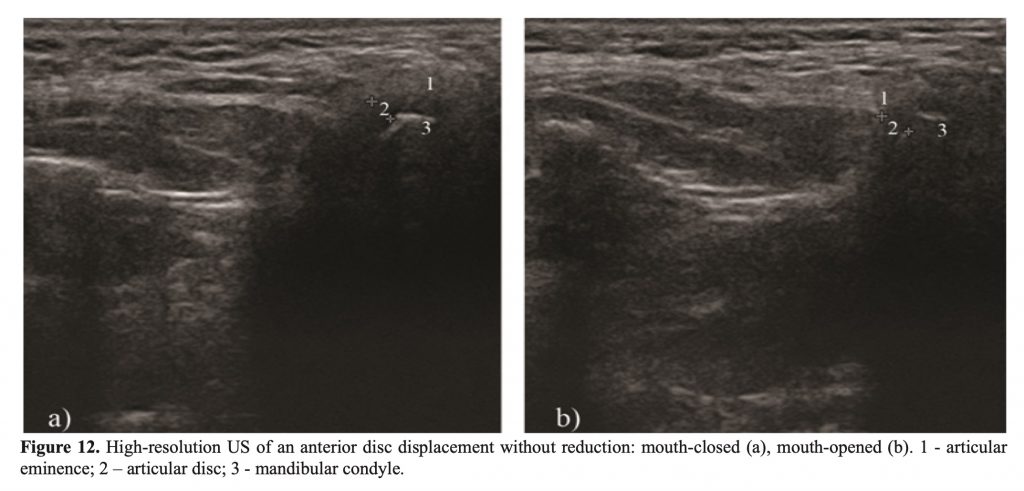
Anteriorly Displaced Disk without Reduction – When a patient opens, there is a tight feeling in the TMJ and there is no click. Patients have a limited opening with Anteriorly Displaced Disk without Reduction.
Often patients with Anteriorly Displaced Disk without Reduction are in significant discomfort. Depending on the severity, sometimes anti-inflammatories help, in some severe cases, even surgery is needed.
Perforated Disk – Patients often hear a grinding sound
Idiopathic Condylar Resorption Diagnosis – ICR or an even better term of Progressive Cindylar Resorption (PCR)
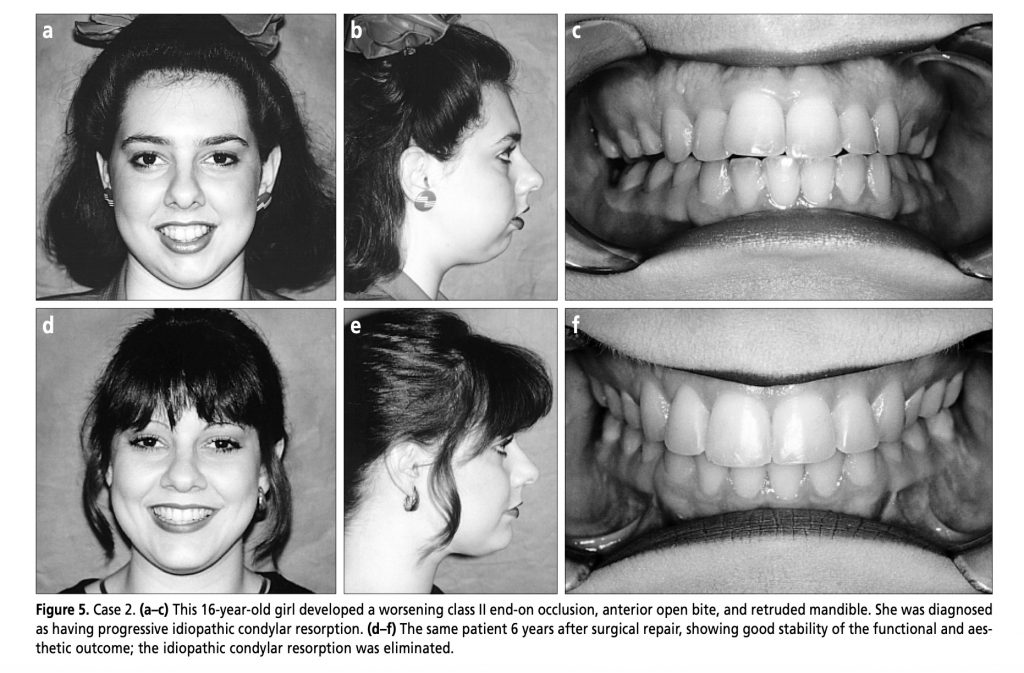
Idiopathic condylar resorption (ICR) is a specific condition that affects the jaw joints (temporomandibular joints or TMJs) and most commonly occurs in teenage girls. It sometimes has been referred to as “cheerleaders syndrome,” because it frequently occurs in teenage girls participating in sports activities which, through minor or major trauma to the jaws, can initiate or exacerbate the condition. ICR is also known as idiopathic condylysis, condylar atrophy, and progressive condylar resorption. This is a well-documented but poorly understood disease process that occurs with a 9:1 female-to-male frequency ratio
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1305829/pdf/bumc0014-0246.pdf
We often see this narrowing and notching of the posterior mandible with ICR cases.


Diagnosis of ICR and PCR.
In general, the following group is considered at high risk for PCR, or ICR.
1. The girls and women of relative low age (<18 years) with
2. anterior open bites,
3. high MPA,
4. short ramus height,
5. low ratio of posterior-to-anterior facial height.
If you notice that your bite is changing, and your bite becoming more class II (more overjet with open bite), and more and more retrognathic (backset) with a progressively larger open bite, usually the best is to rule out ICR by searching for a good experienced OMFS and a trained orthodontists/Dentist.
If a patient has ICR that is active and they have orthognathic jaw correction without addressing the condylar resorption (it is like building a house on running sand), your surgical results can be unstable due to the active condylar resorption. Ask your surgeon about the details.
ICR Diagnoses often is a multi-disciplinary process.
- Sleep study/test to rule out Obstructive Sleep Apnea. Many patients with ICR, and or retrognathia have obstructive sleep apnea. Having a sleep study done can rule out obstructive sleep apnea.
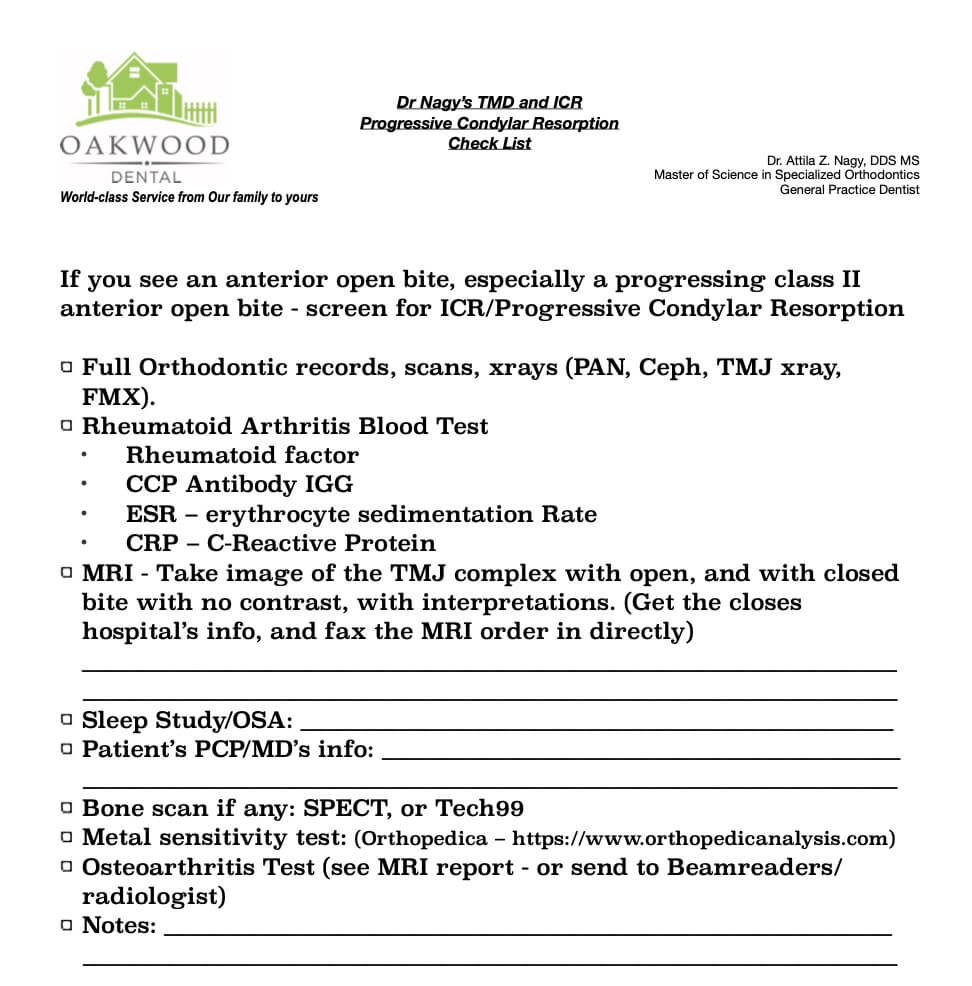
- X-rays: PAN, TMJ x-ray, Ceph
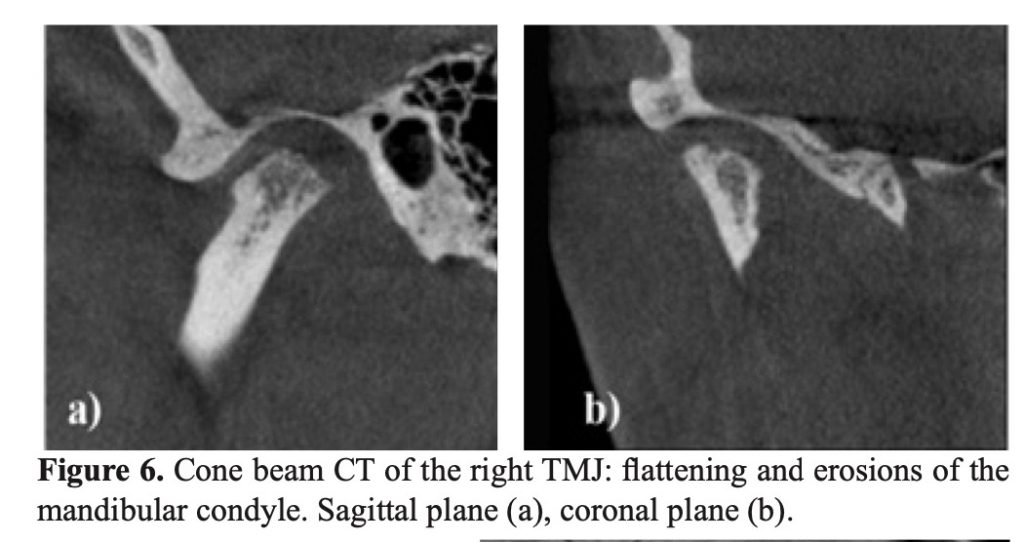
- CBCT – hard tissue and condyle, eminence.
- MRI – Soft tissue such as the TMJ disk.
- Rule out osteoarthritis – wear.
- A blood test to rule out rheumatoid arthritis – inflammatory, and or immunological response. Most Doctors like to order:
- Rheumatoid factor
- CCP Antibody IGG
- ESR – erythrocyte sedimentation Rate
- CRP – C-Reactive Protein
- Metal sensitivity testing (Orthopedica – https://www.orthopedicanalysis.com).
- Bone scan:
- Tech99 (Technetium) nuclear imaging.
- SPECT test: A single-photon emission computerized tomography (SPECT) scan lets your doctor analyze the function of some of your internal organs. A SPECTscan is a type of nuclear imaging test, which means it uses a radioactive substance and a special camera to create 3-D pictures.

Treatment of ICR (ask your surgeon, but here is some basic academic information with reference)
- Mild in-active ICR cases – Stabilize the joint and monitor.
- Moderate to Severe cases – Total TMJ Replacement.
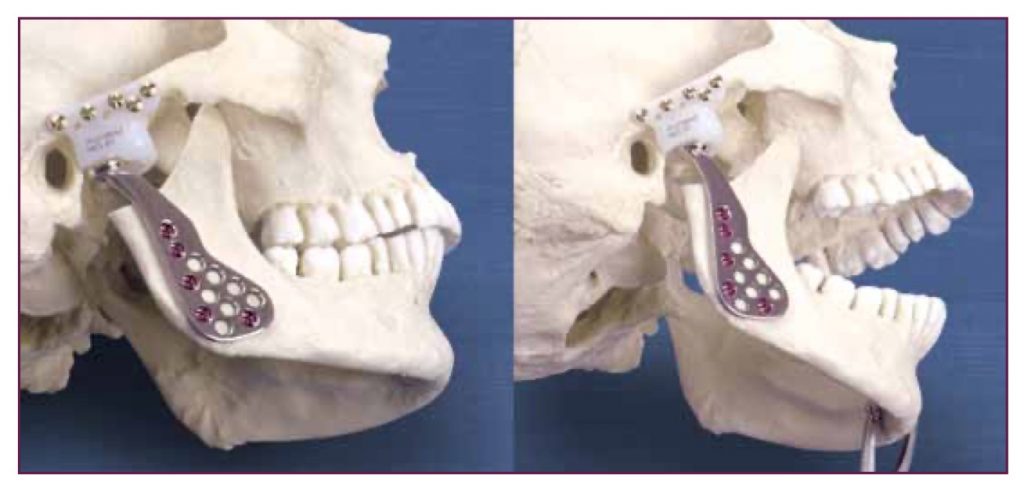
A. Total TMJ replacement.
The Total Temporomandibular Joint (TMJ) Replacement System is implanted in the jaw to functionally reconstruct a diseased and/or damaged temporomandibular joint. The Total TMJ Replacement System is a two-component system comprised of mandibular condyle and glenoid fossa components.
B. TMJ Rib Graft – Less often performed – see literature reference below.
https://synapse.koreamed.org/Synapse/Data/PDFData/3070JKAOMS/jkaoms-40-83.pdf
J Oral Maxillofac Surg. 2019 Sep 14. pii: S0278-2391(19)31075-4. doi: 10.1016/j.joms.2019.09.003. [Epub ahead of print]
Are Rib Grafts Still Used for Temporomandibular Joint Reconstruction?
Hawkins A1, Mercuri LG2, Miloro M3.
Author information
Abstract
PURPOSE:
Patients with end-stage temporomandibular joint (TMJ) pathology require TMJ reconstruction, which can be accomplished with autogenous tissue or alloplastic materials. This survey study evaluates experienced TMJ surgeons’ preferences for autogenous costochondral grafts (CCGs) and/or alloplastic prostheses for TMJ reconstruction.
MATERIALS AND METHODS:
This cross-sectional study used an online public survey domain to query an anonymous cohort of volunteer surgeons from the American and European Societies of Temporomandibular Joint Surgeons about their TMJ reconstruction preferences. The survey questioned these surgeons’ current and previous use of CCG for TMJ reconstruction, changes in practice pattern in this regard over the years, indications for CCG, and postoperative CCG outcomes. The responses were subsequently catalogued, means were calculated, descriptive statistics were analyzed, and trends were identified.
RESULTS:
Of 150 surgeons contacted, 92 responded to the survey. Of the respondents, 84 (91.3%) reported that they had performed total TMJ reconstruction in the past or continue to perform total TMJ reconstruction. However, only the 66 surgeons who completed the survey in its entirety were included in the analysis. Among these surgeons, 95.5% (63 of 66) reported that their current preferred method for TMJ reconstruction was an alloplastic TMJ replacement prosthesis; 86.4% (57 of 66) preferred a custom TMJ prosthesis, whereas 9.1% (6 of 66) preferred a stock TMJ prosthesis. Only 4.5% of the respondents (3 of 66) currently preferred CCG for TMJ reconstruction.
CONCLUSIONS:
Of the respondents, 95.5% preferred alloplastic TMJ replacement. This preference was reported based on fewer postoperative complications and more predictable outcomes using alloplastic TMJ prostheses. In cases in which CCG revision was indicated, an alloplastic TMJ prosthesis was used, indicating that surgeons should consider an alloplastic TMJ replacement device as the primary option for TMJ reconstruction for the management of most end-stage TMJ diseases.